Assessment of harmTable 1 shows the assessment matrix that we designed, which includes all nine parameters of risk, created by dividing each of the three major categories of harm into three subgroups, as described above. Participants were asked to score each substance for each of these nine parameters, using a four-point scale, with 0 being no risk, 1 some, 2 moderate, and 3 extreme risk. For some analyses, the scores for the three parameters for each category were averaged to give a mean score for that category. For the sake of discussion, an overall harm rating was obtained by taking the mean of all nine scores.

The scoring procedure was piloted by members of the panel of the Independent Inquiry into the Misuse of Drugs Act.13 Drugs and the Law, Report of the Independent Inquiry into the Misuse of Drugs Act 1971, The Police Foundation, London (2000).13 Once refined through this piloting, an assessment questionnaire based on table 1, with additional guidance notes, was used. Two independent groups of experts were asked to do the ratings. The first was the national group of consultant psychiatrists who were on the Royal College of Psychiatrists' register as specialists in addiction. Replies were received and analysed from 29 of the 77 registered doctors who were asked to assess 14 compounds—heroin, cocaine, alcohol, barbiturates, amphetamine, methadone, benzodiazepines, solvents, buprenorphine, tobacco, ecstasy, cannabis, LSD, and steroids. Tobacco and alcohol were included because their extensive use has provided reliable data on their risks and harms, providing familiar benchmarks against which the absolute harms of other drugs can be judged. However, direct comparison of the scores for tobacco and alcohol with those of the other drugs is not possible since the fact that they are legal could affect their harms in various ways, especially through easier availability.
Having established that this nine-parameter matrix worked well, we convened meetings of a second group of experts with a wider spread of expertise. These experts had experience in one of the many areas of addiction, ranging from chemistry, pharmacology, and forensic science, through psychiatry and other medical specialties, including epidemiology, as well as the legal and police services. The second set of assessments was done in a series of meetings run along delphic principles, a new approach that is being used widely to optimise knowledge in areas where issues and effects are very broad and not amenable to precise measurements or experimental testing,14 and which is becoming the standard method by which to develop consensus in medical matters. Since delphic analysis incorporates the best knowledge of experts in diverse disciplines, it is ideally applicable to a complex variable such as drug misuse and addiction. Initial scoring was done independently by each participant, and the scores for each individual parameter were then presented to the whole group for discussion, with a particular emphasis on elucidating the reasoning behind outlier scores. Individuals were then invited to revise their scores, if they wished, on any of the parameters, in the light of this discussion, after which a final mean score was calculated. The complexity of the process means that only a few drugs can be assessed in a single meeting, and four meetings were needed to complete the process. The number of members taking part in the scoring varied from eight to 16. However, the full range of expertise was maintained in each assessment.
This second set of assessments covered the 14 substances considered by the psychiatrists plus, for completeness, six other compounds (khat, 4-methylthioamphetamine [4-MTA], gamma 4-hydroxybutyric acid [GHB], ketamine, methylphenidate, and alkyl nitrites), some of which are not illegal, but for each of which there have been reports of abuse (table 2). Participants were told in advance which drugs were being covered at each meeting to allow them to update their knowledge and consider their opinion. Recent review articles[5], [6], [7], [15], [16], [17] and [18] were provided.
--------------------------------------------------------------------------------
Table 2.
The 20 substances assessed, showing their current status under the Misuse of Drugs Act

Occasionally, individual experts were unable to give a score for a particular parameter for a particular drug and these missing values were ignored in the analysis—ie, they were neither treated as zero nor given some interpolated value. Data were analysed with the statistical functions in Microsoft Excel and S-plus.
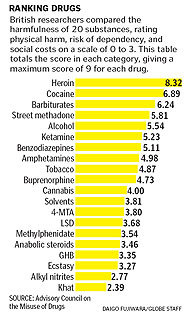
ResultsUse of this risk assessment system proved straightforward and practicable, both by questionnaire and in open delphic discussion. Figure 1 shows the overall mean scores of the independent expert group, averaged across all scorers, plotted in rank order for all 20 substances. The classification of each substance under the Misuse of Drugs Act is also shown. Although the two substances with the highest harm ratings (heroin and cocaine) are class A drugs, overall there was a surprisingly poor correlation between drugs' class according to the Misuse of Drugs Act and harm score. Of both the eight substances that scored highest and the eight that scored lowest, three were class A and two were unclassified. Alcohol, ketamine, tobacco, and solvents (all unclassified at the time of assessment) were ranked as more harmful than LSD, ecstasy, and its variant 4-MTA (all class A drugs). Indeed, the correlation between classification by the Misuse of Drugs Act and harm rating was not significant (Kendall's rank correlation −0·18; p=0·25; Spearman's rank correlation −0·26, p=0·26). Of the unclassified drugs, alcohol and ketamine were given especially high ratings. Interestingly, a very recent recommendation from the Advisory Council on the Misuse of Drugs that ketamine should be added to the Misuse of Drugs Act (as a class C drug) has just been accepted.19

Figure 1. Mean harm scores for 20 substances
Classification under the Misuse of Drugs Act, where appropriate, is shown by the colour of each bar.
We compared the overall mean scores (averaged across all nine parameters) for the psychiatrists with those of the independent group for the 14 substances that were ranked by both groups (figure 2). The figure suggests that the scores have some validity and that the process is robust, in that it generates similar results in the hands of rather different sets of experts.

Figure 2. Correlation between mean scores from the independent experts and the specialist addiction psychiatrists
1=heroin. 2=cocaine. 3=alcohol. 4=barbiturates. 5=amphetamine. 6=methadone. 7=benzodiazepines. 8=solvents. 9=buprenorphine. 10=tobacco. 11=ecstasy. 12=cannabis. 13=LSD. 14=steroids.
View Within Article
Table 3 lists the independent group results for each of the three subcategories of harm. The scores in each category were averaged across all scorers and the substances are listed in rank order of harm, based on their overall score. Many of the drugs were consistent in their ranking across the three categories. Heroin, cocaine, barbiturates, and street methadone were in the top five places for all categories of harm, whereas khat, alkyl nitrites, and ecstasy were in the bottom five places for all. Some drugs differed substantially in their harm ratings across the three categories. For instance, cannabis was ranked low for physical harm but somewhat higher for dependence and harm to family and community. Anabolic steroids were ranked high for physical harm but low for dependence. Tobacco was high for dependence but distinctly lower for social harms, because it scored low on intoxication. Tobacco's mean score for physical harm was also modest, since the ratings for acute harm and potential for intravenous use were low, although the value for chronic harm was, unsurprisingly, very high.
--------------------------------------------------------------------------------
Table 3.
Mean independent group scores in each of the three categories of harm, for 20 substances, ranked by their overall score, and mean scores for each of the three subscales

Drugs that can be administered by the intravenous route were generally ranked high, not solely because they were assigned exceptionally high scores for parameter three (ie, the propensity for intravenous use) and nine (health-care costs). Even if the scores for these two parameters were excluded from the analysis, the high ranking for such drugs persisted. Thus, drugs that can be administered intravenously were also judged to be very harmful in many other respects.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}